
Anna Elzabeth Tom, Correspondent, India Pharma Outlook

Every Mother’s Day, the world celebrates motherhood with cards, flowers and images of glowing mothers. World portrays motherhood as a period of happiness, but for millions of mothers, this may be far from truth. Behind all these celebrations in every seven new mothers are struggling silently with something they don’t talk about much, Postpartum Depression.
You just had your baby. You see your little one sleeping in your arms. Your loved ones are happy; they are telling you how cute your baby is. You smile back at them and act happy, because this is what the world expects from you. But on the inside, you feel nothing, and you are embarrassed and feel guilty about this. This is what postpartum depression looks like: a mother sitting in the middle of everyone's happiness, feeling empty, alone, and ashamed of herself.
Post-Partum Depression or PDD is a clinical mood disorder following childbirth. It’s a medical condition that occurs when our brain struggles to adapt to the hormonal and neurological shifts that happen after birth.
Tiffany R. Farchione, M.D., director of the Division of Psychiatry, FDA’s Center for Drug Evaluation and Research states “Postpartum depression is a serious and potentially life-threatening condition in which women experience sadness, guilt, worthlessness—even, in severe cases, thoughts of harming themselves or their child. And, because postpartum depression can disrupt the maternal-infant bond, it can also have consequences for the child’s physical and emotional development.”
During pregnancy, the progesterone level in women rises sharply and is broken into allopregnanolone (ALLO), a neurosteroid that helps in regulating anxiety and keeping it at bay. Similarly, Estrogen regulates serotonin and dopamine, which control the mood, keeping the pregnant woman stable. But immediately after the delivery, progesterone and estrogen levels fall, and this cuts down the supply of allopregnanolone, disrupting brain activity and finally triggering PPD.
The postpartum period begins one hour after delivery and extends for a period of 42 days. Clinically, this has three phases, starting with the acute phase, which lasts for 12 hours post-delivery, followed by the sub-acute phase spanning over to the next six weeks, and the delayed phase from six weeks to six months when gradual recovery happens. PPD usually starts in the sub-acute phase and if left unchecked can last up to 12 months.
Also Read: Infertility in India: Challenges and New Hope Ahead
Not every postpartum mood disorder is the same. There mainly three types of post-partum mood disorders based on their varying severity.
About 50 to 85 percent of new moms experience baby blues in the first few weeks following delivery. It’s normal and is not a severe mental illness. The mother may feel anxiety, sadness ad irritability, and it usually peaks on the fourth or fifth day post-delivery and should usually subside within two weeks.
On the other hand, postpartum depression is persistent and doesn’t subside after two weeks. One in every seven new mother has been shown to develop PDD. It can extend for months and will affect the daily functionality of the mother. The mother develops anxiety, a change in appetite and sleep, hypochondriasis, and even suicidal tendencies.
“You can expect a little baby blues in some women for certain, but with postpartum depression, when a patient has persistent sadness, a loss of interest in pleasure, and anhedonia, and it is really affecting her quality of life…” says Deb York, MSN, PMHNP-BC, APRN, CCRA, Adjunct Faculty Instructor, Walden University.
Postpartum obsessive-compulsive disorder has also been reported, where women start having intrusive thoughts of killing their infants. The most severe postpartum mental disorder is Postpartum Psychosis. It’s usually rare, and only one or two in 1000 new mothers experience this. This is a psychiatric emergency, and the mother experiences hallucinations, insomnia, bipolar episodes, irritability and delusions. Women with Postpartum Psychosis are at high risk of suicide and infanticide.
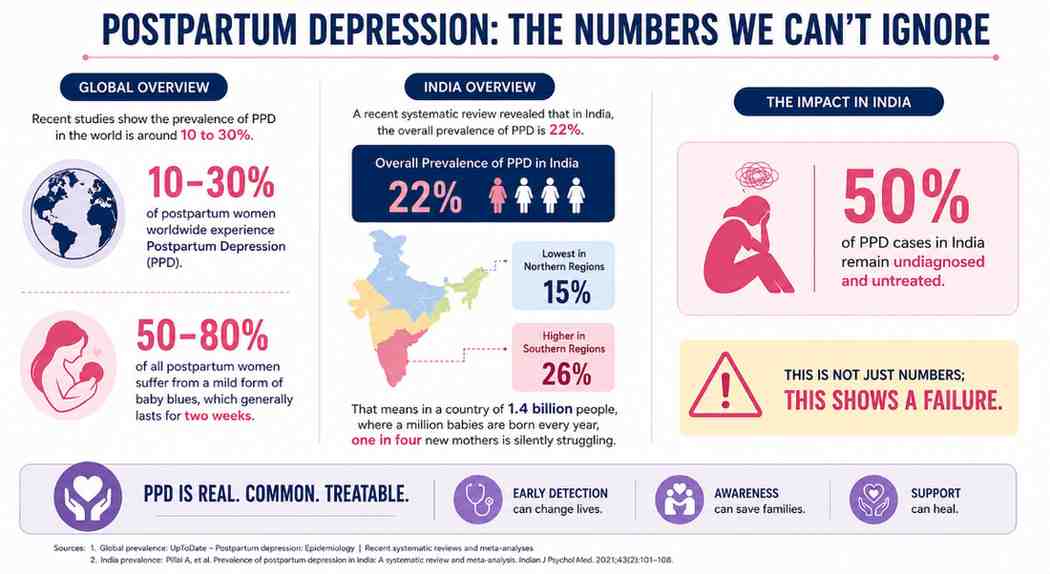
Recent studies revealed a shocking truth that we should not ignore. Recent studies show that the prevalence of PPD in the world is around 10 to 30%. Nearly 50 to 80% of all postpartum women suffer from a mild form of baby blues, which generally lasts for two weeks.
A recent systematic review revealed that in India, the overall prevalence of PPD is 22%. The southern regions showed greater prevalence (26%) and the lowest in northern regions (15%). That means in a country of 1.4 billion people, where a million babies are born every year, one in four new mothers is silently struggling. And yet, 50% of these cases remain undiagnosed and untreated in India. This is not just numbers; this shows a failure.
But why has this stayed in the shadows for so long? One of the reasons is that for decades, postpartum care has primarily focused on the infant's health and weight while the mother sat quietly suffering in silence. The mother was expected to be happy and grateful if the infant was healthy. A woman complaining of anxiety would have been overlooked or labeled hysterical. And as a result, generations of new mothers suffered alone.
For decades, postpartum depression was treated just like any other common depression, and the go to solution was antidepressants. Selective Serotonin Reuptake Inhibitors (SSRI) such as sertraline (Zoloft) and fluoxetine (Prozac), serotonin-norepinephrine reuptake inhibitors (SNRIs) like duloxetine and desvenlafaxine and tricyclic antidepressants thus became the default remedy.
They helped some women, but they were not designed for Postpartum Depression. They were designed for treating general depression syndrome and not specifically the neurological and hormonal events that occurs post childbirth. And they take four to six weeks to start showing improvement and for a new born mother alone dealing with an infant and depression it feel like an eternity.
These antidepressants also carry along with it a plethora of side effects like nausea, insomnia and sexual dysfunction. In extreme conditions, it can also lead to antidepressants discontinuation syndrome, seizures and serotonin syndrome. For a new mother who is dealing with physical, emotional and lifestyle changes these side effects can be very horrifying.
In 2019, the first breakthrough in Postpartum Depression (PPD) happened when the FDA approved brexanolone, sold as Zulresso; the first-ever drug developed specifically for postpartum depression. It is a chemically identical formulation of allopregnanolone itself, thus restoring the lost hormone and providing relief much faster in about 48 hours post medication.
But this quick relief comes at a very high price. It is administered as a continuous intravenous infusion for 60-hours at a certified healthcare facility. The patient is continuously monitored throughout the entire process due to the risk of serious side effects like sedation, vertigo, and sudden loss of consciousness. It might also lead to hypoxia (oxygen deficiency).To avail the medication; the patient should be enrolled in the Risk Evaluation and Mitigation Strategy (REMS) program.
Women who received it reported that they started to feel like themselves within a few days. It was a historic moment, because for the first time, women with postpartum depression were feeling better in days and not in weeks.
But here’s the reality check: a single vial of brexanolone costs roughly around USD 7,450, and an average treatment requires around four and a half vials, thus raising just the cost of medication to around USD 30,000 to 34,000. For an average Indian woman, just spending 28 to 30 lakhs for a depression just feels out of reach. And moreover, this medication is only available in the United States under a restricted programme in a specialized facility. The medicine is not available for routine clinical use in India. So for the vast majority of global women, this medicine is still out of their reach.
On August 4, 2023, came the next great leap for postpartum depression, Biogen’s zuranolone, branded Zurzuvae was approved by the U.S. Food and Drug Administration. On the occasion of approval of the medicine, Priya Singhal, Head of development, Biogen remarked “This approval is a major milestone in addressing a critical unmet need in maternal health for women in Europe, where postpartum depression is underdiagnosed and undertreated.”
Zuranolone works using the same neurosteroid mechanism as brexanolone. But, unlike brexanolone it’s in the form of a capsule that can be orally taken. The recommended dose for Zuezuvae is 50mg per day, and it has to be taken for a period of 14 days in the evening following a fatty meal. This was a ray of hope for many women. Now, they could take the medicine from their homes without getting hospitalized and needing an IV Line.
But again, this is not widely available in India via local pharmaceutical companies. One require a specialized named-patient import to access the medicine and it costs around Rs11,000 to Rs 22,000 and above for a pack of 14 capsules excluding import permit charges.
Things are getting better, but the work is far from over. These medicines are not safe for everyone and they remain inaccessible to most women around the world. To make the benefit reach the women who need it the most a lot of effort needs to be done on cost, infrastructure and creating awareness. The greatest gift we can give our mothers is not just love, but the certainty that they will not be left alone.





 Through Collaborative Efforts")
, CDSCO.jpg "Fostering a Quality Culture in the Pharmaceutical Industry")