
Zeenat Parween, Correspondent, India Pharma Outlook

In early May 2026, hospital workers in Bunia, Northeastern Congo, started falling sick. Lab tests came back negative for Ebola — then a second round told a very different story.
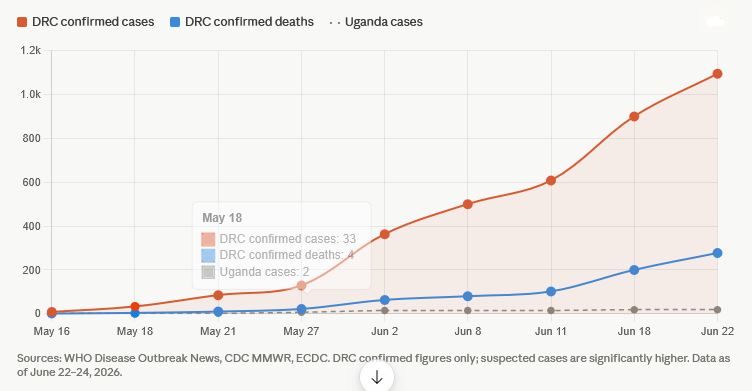
Eight out of 13 samples tested positive for the Bundibugyo virus — a rare, lethal strain of Ebola virus disease. What followed was fast, alarming, and still unfolding. By June 22, the DRC had confirmed over 1,094 cases, making this the second largest Ebola outbreak in recorded history. Cases rose faster here than in any previous Ebola outbreak, prompting growing concern among global health experts.
The virus did not stay contained. By mid-May it had crossed into Uganda's capital Kampala. A US doctor was evacuated to Germany. France confirmed a case on June 24. On May 17, the WHO declared a Public Health Emergency of International Concern — the same highest-level alarm used for COVID-19.
 Ebola spreads through direct contact with body fluids like blood, saliva and sweat of someone already sick or who has died. It does not travel through air. That sounds manageable, until you look at what is happening on the ground.
Ebola spreads through direct contact with body fluids like blood, saliva and sweat of someone already sick or who has died. It does not travel through air. That sounds manageable, until you look at what is happening on the ground.
The world has a licensed Ebola vaccine, ERVEBO, but it only protects against the Zaire strain. The Bundibugyo virus is different, and nothing currently approved can stop it. Past Bundibugyo outbreaks had death rates of 32 percent and 55 percent respectively.
Experts believe the first human infections may have occurred as far back as February 2026, in Mongbwalu — a busy mining town in Ituri. By the time the outbreak was formally declared in May, it had been spreading undetected for roughly three months.
Ituri Province borders both Uganda and South Sudan. Miners, traders, and displaced families cross these borders daily. Armed conflict in the region blocks surveillance teams and makes contact tracing nearly impossible.
The initial cluster hit hospital staff in Bunia — a sign of missed detection. When doctors and nurses fall ill, it doesn't just reduce the response workforce. It shuts down trust in the health system entirely.
Maria Van Kerkhove, WHO's Acting Director of Epidemic and Pandemic Preparedness, said: "Good early clinical care saves lives, even without specific treatment."
Also Read: Ebola Cases Cross 1,000 Mark as WHO Issues Fresh Warning
CDC modelling from June 2026 showed that with only 20 percent of sick patients isolated, there is a 65 percent chance the outbreak exceeds 20,000 cases within three months. The agency called for a response comparable in scale to the 2014–2016 West Africa Ebola epidemic, which killed over 11,300 people and took nearly two years to control.
Ituri Province has 997 confirmed cases across 22 health zones. North Kivu has added 94 more from 11 health zones. The count keeps rising — 46 new cases were added in a single day on June 23. This is the DRC's 17th Ebola outbreak since 1976, starting just five months after the previous one ended.
CEPI has committed over USD 60 million toward three experimental Bundibugyo vaccines. Moderna's mRNA candidate received up to USD 50 million. The University of Oxford's ChAdOx1 candidate — built on the same platform as the AstraZeneca COVID-19 vaccine — received USD 8.6 million, with manufacturing assigned to India's Serum Institute of India (SII).
Adar Poonawalla, CEO of the Serum Institute of India, said: "At moments like this, speed, scale and access is all that matters. SII will bring its manufacturing capabilities to this collaboration with CEPI and the University of Oxford to help advance a Bundibugyo virus vaccine candidate as quickly as possible."
The Oxford-SII candidate could be ready for clinical trials within two to three months — the fastest timeline among candidates in development. On treatment, WHO adviser Salim S. Abdool Karim said remdesivir, if proven effective, could be "a strong weapon" given it is widely available and affordable in generic form.
Uganda confirmed its first case on May 15 — a traveller from Ituri who died before the outbreak was even formally declared. A second, unlinked case appeared the next day. As of June 18, Uganda has reported 19 confirmed cases, all linked to Kampala and Wakiso district, with no documented community transmission.
This is Uganda's ninth Ebola outbreak. That experience showed: the national Ebola Treatment Unit at Mulago Hospital was operational within six hours of the outbreak declaration. The Emergency Medical Team of 146 members deployed within two.
WHO Director-General Dr. Tedros Adhanom Ghebreyesus visited Uganda in early June and cautioned against travel bans: "Travel bans are not helpful in controlling Ebola outbreaks and can negatively affect the movement of essential supplies, response teams and commodities needed to support control efforts."
Other Countries Reporting Ebola Cases or Imported Infections
France confirmed Europe's first imported Ebola  case on June 24 — a doctor who had been on a humanitarian mission in the DRC and returned home showing symptoms. The case was not acquired in France; there is no chain of local transmission. French health authorities moved quickly to isolate the patient and trace contacts.
case on June 24 — a doctor who had been on a humanitarian mission in the DRC and returned home showing symptoms. The case was not acquired in France; there is no chain of local transmission. French health authorities moved quickly to isolate the patient and trace contacts.
An American physician treating patients at Nyankunde hospital in Ituri tested positive for Bundibugyo Ebola in May. Along with his wife and children, he was medically evacuated to Berlin's Charité Hospital — one of Europe's foremost infectious disease facilities. He received antiviral therapy and experimental monoclonal antibodies. The family was released on June 6 after making a full recovery. No secondary cases were recorded.
No Ebola cases have been confirmed on US soil. However, the response has been significant. The CDC issued a Level 3 Travel Health Notice for DRC and a Level 1 Notice for Uganda. All travellers from DRC, Uganda, and South Sudan within the past 21 days must now enter the US only through four designated airports — Washington Dulles, Atlanta, Houston, and JFK — for enhanced screening.
The State Department deployed a Disaster Assistance Response Team to DRC within four days of the first case notification, described as the fastest-ever DART deployment for a US Ebola response. Total US funding committed has exceeded USD 220 million in direct Ebola response, with a further USD 350 million in humanitarian assistance to the region.
The UAE has not reported any confirmed Ebola cases, but its position as a major global transit hub — particularly through Dubai — puts it in a unique position. Emirates airline issued a travel advisory. Dubai's airports serve as a key connecting point for passengers travelling between Africa and Asia, including India. US-funded humanitarian supplies bound for Uganda have also transited through Dubai.
On May 22, a patient who had recently visited DRC-affected areas was hospitalised in the Netherlands with symptoms compatible with Ebola. The case was investigated under precautionary protocols, though it underscored that EU health systems must remain alert to returning travellers from affected regions. The ECDC's operational checklist, published in June 2026, was designed specifically to help EU member states respond swiftly to exactly these scenarios — even when cases ultimately test negative.
Also Read: E-pharmacy in India 2026: Top Apps for Medicine Delivery
In account to the Ebola surveillance, Canada, Bahamas has strictly declared the temporary ban on residents of DRC, Uganda, and South Sudan. This states that residents from those countries would be unable to travel to Canada for 90 days.
Similarly, the Bahamian government with respect to the Ebola monitoring efforts, restricted travelers for a period of 30 days. The US has also came with restrictions, banning all the non-citizens travelled to DRC, Uganda, and South Sudan in the previous 21 days.
Later the CDC expanded the ban to the green card holders who has visited the countries at risk of Ebola. Consequently US also asked the travelers who visited the affected countries to return to the US airports that are equipped with effective screening.
As per the reports no cases of Ebola has been reported in countries like Canada, Bahamas, and US. Whereas India with respect to the Ebola monitory efforts has setup effective screening measures at major International airports.
Countries such Rwanda, Kenya, South Sudan, Tanzania, Burundi, yet has no reported cases. But these are on high alert due to the proximity to DRC. Therefore as per reports Kenya and Tanzania has initiated screening process along with tracing protocols with respect to outbreak preparedness.
Amid on the concern on the outbreak, Union Health Minister, Jagat Prakash Nadda has reviewed on India’s preparedness on Ebola. India has arranged effective screening measures at the major airports.
India has also issued a travel advisory, stating that citizens should avoid non-essential travels to DRC, Uganda and South Sudan. Union Minister also confirms that there are no present imported cases on Ebola in India.
India has also installed Integrated Disease Surveillance Program (IDSP) units and the Airport Health Organization is instructed to strengthen the vigilance unexplained illness among international travellers.
Due to severity of issue, New Delhi has also postponed the India-Africa Summit scheduled to host in the consecutive weeks. Reports say that they have also called of International Big Cat Alliance, led by India of 95 members, which include members of alliance from South Africa.
Also India has previous lessons on several infectious outbreaks from Nipah, Dengue, to Covide-19 pandemic. Therefore this calls for critical action o and proper monitoring on Ebola surveillance in India, as India is highly vulnerable to imported diseases.
due to the massive International travel hubs, and high population density in India, the risk of imported diseases are high. Therefore to tackle India launches Air Suvidha 2.0, a full contact-less health declaration portal for travellers.
India has brought back Air Suvidha in an upgraded digital form. Air Suvidha 2.0 is now mandatory for all international passengers arriving in India, with travelers required to submit an online Health Self-Declaration form up to 24 hours before arrival.
The system gives health and immigration officials access to passenger details in real time, helping them spot possible risks faster. The move is meant to improve airport screening and shows how countries are tightening border health checks as the Ebola outbreak raises global concern.
The 2026 Ebola outbreak is more than a regional health emergency. It is a reminder of how quickly infectious diseases can move across borders in an interconnected world. While the outbreak began in the Democratic Republic of the Congo, imported cases in Europe and growing international travel concerns have transformed it into a global public health issue.
What makes this outbreak particularly concerning is the involvement of the Bundibugyo strain, for which there is currently no approved vaccine or targeted treatment. Delayed detection, cross-border movement, conflict-affected regions, and pressure on healthcare systems have further complicated containment efforts.
At the same time, the response offers important lessons. Countries with prior Ebola experience, such as Uganda, have demonstrated the value of rapid preparedness, while international organizations and vaccine developers have accelerated efforts to prevent a wider crisis.
For India and other nations with extensive global connectivity, the outbreak highlights the need for constant vigilance, strong surveillance systems, and coordinated public health responses. The story is not only about Ebola's spread today but also about the world's ability to detect, contain, and respond to the next infectious threat before it becomes a larger crisis. Also, India's decision to roll out Air Suvidha 2.0 reflects a broader global trend of strengthening public health surveillance at international borders as countries remain alert to the evolving Ebola situation.
The coming months will determine whether this outbreak remains a severe regional emergency or evolves into a broader international challenge. Until then, preparedness, transparency, and global cooperation remain the most effective tools available.





 Through Collaborative Efforts")
, CDSCO.jpg "Fostering a Quality Culture in the Pharmaceutical Industry")